Table Of Content
We have included three studies of this nature in this review [12,14,17] although it is questionable whether studies with only two steps should be considered as stepped wedge designs. Figure Figure22 shows the results of our search which identified only 12 papers or protocols (referred to as studies) in which a stepped wedge design was described. Three of the included studies [12-14] are protocols describing trials that were being designed or implemented rather than providing results of the evaluation. Basic information about each of the included studies is shown in Tables Tables1,1, ,2,2, ,33. The review includes studies based on both individual and cluster allocations and is not restricted to RCTs.
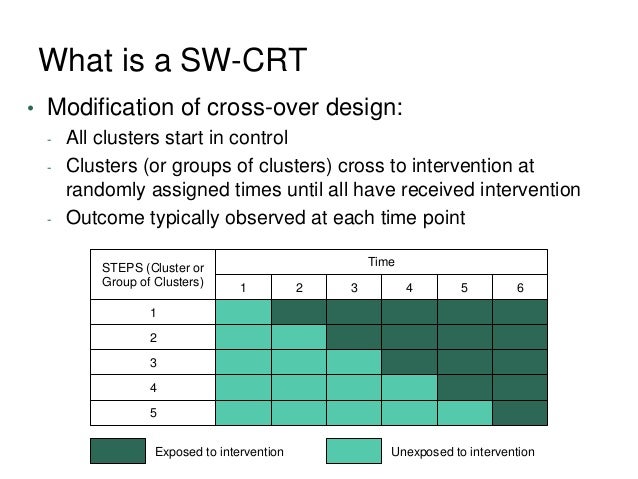
Designing a stepped wedge trial: three main designs, carry-over effects and randomisation approaches
Here we assume a complete design, meaning that data are collected from each cluster throughout the trial. In the next section we consider incomplete designs and analysis approaches, which can allow more flexible choice of the length and number of steps. The first was conducted by Stern et al., and could be characterised as having continuous recruitment followed by long and varying periods of exposure [12].
Side Swept Bangs
He received his Ph.D. in biostatistics from the University of North Carolina at Chapel Hill. Prior to arriving at Yale, Dr. Zhou was a Postdoctoral Fellow in the Departments of Biostatistics and Epidemiology at Harvard T.H. Chan School of Public Health. His research focuses on cluster randomized trials, measurement error correction, and statistical and machine learning methods in precision medicine. There is risk of cross-contamination between sites in different phases of the study (eg, across sequences), especially if sites are from the same network or geographic region. The Virginia cooperative, which used SW-CRT design, opted to randomize groups of practices as a block to contain any cross-talk within sequences.
How the stepped wedge cluster randomised trial relates to other cluster designs
Comparison of analysis methods and design choices for treatment-by-period interaction in unidirectional switch ... - BMC Medical Research Methodology
Comparison of analysis methods and design choices for treatment-by-period interaction in unidirectional switch ....
Posted: Thu, 17 Nov 2022 08:00:00 GMT [source]
Single measurement, repeated measurements or time-to-event from the start of the individual’s exposure may be chosen to assess outcomes, depending on the research question. Trials should generally not commit resources to collect outcome data from individuals exposed a long time before or after the rollout period. Though substantial carry-over effects are uncommon in stepped wedge trials, researchers should consider their possibility before conducting a trial with closed or open cohorts. It is also important to note that the stepped wedge design is likely to lead to a longer trial duration than a traditional parallel design, particularly where effectiveness is measured immediately after implementation. Blinding assessors is particularly important since it is almost impossible to blind participants or those delivering the intervention, since both will be aware of the 'step' from control to intervention status. As will be shown in this paper, a variety of approaches to statistical analysis have been employed empirically, in part due to the complex nature of the analysis itself.
The stepped wedge cluster randomised trial offers a randomised method of evaluation of an intervention delivered at the level of the cluster. In cases where randomisation to either control or intervention arm is precluded but randomisation to a date of initiation is possible, it offers a means of a randomised evaluation in place of a less robust design. However, the design requires the fitting of more complex models than parallel designs and must adjust for underlying temporal trends.
Authors’ original submitted files for images
However, there were many organizational arguments against this, so the SWD design was chosen. Compared to mixed-effects models, a caveat of marginal models is that the robust standard errors may exhibit negative bias with a limited number of clusters (often not exceeding 30). Computational challenges in GEE methods for CRTs with large cluster sizes have also been investigated in Chen et al.48 with a stochastic GEE and Li et al.37 with an efficient cluster-period GEE method. Key considerations are discussed including mainstream methods of analysis and sample size determination. Finally, a stepped wedge design also allows exploration of heterogeneity in treatment effects between clusters, using within cluster comparisons of exposed and unexposed periods. Although the design may not be powered for these analyses, they can inform an interesting secondary investigation.
Defining characteristics of stepped wedge cluster randomised trials, allocation and terminology
And Ph.D. students in Epidemiology and teaches Biostatistics courses at the University of Ottawa. The grantees reported possible data quality issues owing to suspected Hawthorne effects, which is a related but novel finding. The SW-CRT design involves lags between when sites are recruited, randomized, and receive the intervention, leading to site-retention challenges. Some cooperatives experienced attrition between recruitment and randomization; the Northwest cooperative reported that 47 sites dropped out by the time all partnership agreements were signed and sites randomized. Others lost sites randomized to later sequences, which involved waiting more than a year before starting the intervention. Cooperatives with recruitment networks in place were able to shift efforts from recruitment to retention.
Sample Size Determination
In such trials we consider outcome data from individuals exposed before, during, or after rollout to be ‘collected’ before, during, or after rollout. The value of the principle of randomization to compare treatments and interventions remains undisputed in medical research, and randomized controlled trials (RCTs) are the acknowledged gold standard. Due to practical considerations, a number of variations have been developed in addition to the traditional RCT design, including cluster-randomized trials and the stepped-wedge design (SWD). In cluster-randomized, parallel-group trials—the prevailing type of cluster-randomized trial—groups of individuals (e.g. doctors’ practices, school classes, regions), rather than individuals themselves, are randomized to receive the intervention.
Carry-over effects may also seem unlikely because in some SWT the control condition exists in the population before the trial, and so all participants have already been exposed to the control for so long that some additional exposure during the trial is unimportant. In the design literature [2], the ‘classic’ SWT design includes one step length of data collection before rollout and one step length of data collection after rollout, as in case study one. There are two reasons why we do not, in general, recommend collecting (and then including in the primary analysis) more data from longer periods before or after rollout, particularly if this uses resources that could be used to collect more data during the rollout period.
Where there are a small number of steps, these characteristics can be compared by randomisation group (as in example 3). This should include the numbers analysed, the average cluster size, cluster characteristics, and important patient characteristics. The actual design, showing numbers of observations per cluster, can be schematically presented, as shown in fig 3⇓. Evaluation of drug therapies has long been deemed essential in accordance with evidence based medicine. The evaluation of non-pharmaceuticals, such as policy changes or service delivery methods, has unfortunately been less rigorously evaluated.
One reason for this is the limitations for generalisation, particularly with respect to the impact of time on effectiveness. Figure 2 shows the results of our search which identified only 12 papers or protocols (referred to as studies) in which a stepped wedge design was described. The studies included in the review described their study design as either stepped wedge or phased introduction/implementation. We contacted the authors of the conference proceeding report identified by a citation check and a protocol identified by the Controlled Trials Register but were unable to obtain sufficient information about these trials to include them in our review.
This eBox compares sample cluster-randomized SWD and parallel-group trials in various scenarios in which both the variance s2 of cluster means and their correlation ? Between times at which the outcomes are measured depend on the intraclass correlation coefficient (ICC) within clusters. While the small sample makes generalisations difficult, the stepped wedge design appears to be primarily used in evaluating interventions in developing countries, with HIV the most common disease addressed (Table (Table1).1). Table Table22 identifies that a number of different interventions were being evaluated, with vaccination, screening and education plans emerging as the most common interventions. In the remaining four studies with both 'intervention' and 'control' participants [4, 12, 21, 22], the unit of randomisation is the clinic or ward and hence an individual visiting the clinic/ward while it is in the control section of the wedge will not receive the intervention.
Challenges included (1) time-sensitive recruitment, (2) retention, (3) randomization requirements and practice preferences, (4) achieving treatment schedule fidelity, (5) intensive data collection, (6) the Hawthorne effect, and (7) temporal trends. PURPOSE Despite the growing popularity of stepped-wedge cluster randomized trials (SW-CRTs) for practice-based research, the design’s advantages and challenges are not well documented. The objective of this study was to identify the advantages and challenges of the SW-CRT design for large-scale intervention implementations in primary care settings. In order for SWT designs to be fully reported and to enable readers to judge their strengths and weaknesses, it is important to describe how individuals participate in a trial, how they are exposed to control and/or intervention conditions, and how measurements are obtained. In a recent article, Hemming et al. described three SWT designs, but these mainly considered how measurements are obtained from individuals, and not features of participation or exposure [8]. We first describe three common designs for SWTs identified in our review of 37 trials, then briefly outline characteristics by which the individual participation exposure and measurement can be identified and reported in an SWT.
CONCLUSIONS The challenges experienced by EvidenceNOW grantees suggest that certain favorable real-world conditions constitute a context that increases the odds of a successful SW-CRT. Strong retention plans are needed to continue to engage sites waiting to start the intervention. Finally, study outcomes should be ones already captured in routine practice; otherwise, funders and investigators should assess the feasibility and cost of data collection. As a biostatistician, Dr. Li works with researchers from a variety of medical specialties in the design and analysis of cluster randomized trials, individually randomized clinical trials, and observational studies. And Ph.D. students in biostatistics and teaches a course on causal inference methods at Yale University School of Public Health. In case study three it seems most data included in analysis were collected before or after the rollout period.
Carry-over effects can also arise at the cluster level in trials comparing methods to detect a health condition and change its management. In such a scenario, the number of undetected cases remaining in clusters may decline over time. The types of undetected cases may also change, for example because cases that are more challenging to identify might remain undetected longer. The intervention and control conditions could therefore differ in how effectively cases are detected, and these changes over time will be influenced by the duration of the control condition.
Two approaches can be taken to shorten the step length, and possibly also total trial length, albeit potentially resulting in requiring more clusters in the trial. The first is to acknowledge the lag at the analysis stage [14], and is discussed by trialists in our companion paper [15]. Another solution at the design stage is to not collect data from clusters during the lag period, an incomplete design represented in Fig. If measurements are taken before crossover points in a closed or open cohort SWT, then this approach allows the step length as selected for a complete SWT to be halved, as now we wish two step lengths to be greater than the lag period. This use of an incomplete design is worthy of consideration whenever there is a lag, that is, if the step duration for a complete SWT is longer than desired. Stepped wedge cluster randomized trials enable rigorous evaluations of health intervention programs in pragmatic settings.







No comments:
Post a Comment